


This is a short clip from Masters Mahan Podcast Episode #09 - Principal #4 of Satanic Human Control & Enslavement: To Survive At Any Cost

Watch the Full Episode #09 in Video Format
Watch Episode(s) #05-10 which Cover Principal(s) #01-05 of Satanic Human Control (MkUltra / Monarch Program)
This is just an edit of Episode(s) #05-10 put together since they are part of a single sub-series topic of the podcast.

A Brief Introduction to the Work of Dr. Peter Breggin
“Peter R. Breggin, M.D., is a psychiatrist and expert in clinical psychopharmacology. A former teaching fellow at Harvard Medical School and full-time consultant at the National Institute of Mental Health, he has written dozens of scientific articles and more than twenty books, including the bestsellers Toxic Psychiatry and Talking Back to Prozac. He has served as a medical expert in criminal and civil cases involving psychiatric drugs, including product-liability suits against drug manufacturers. Dr. Breggin founded the International Center for the Study of Psychiatry and Psychology, taught at universities, and is on the editorial boards of several scientific journals. He lives in the Finger Lakes region with his wife, Ginger, and practices psychiatry in Ithaca, New York.” (Source)
Dr. Peter and Ginger Breggin on Substack

Dr. Breggin Heavily Advocated for the Banning of Lobotomy [in the USA] during the 60s-70s
Stopping the Resurgence of Lobotomy and Psychosurgery
After completing medical school, internship and three years of psychiatric residency training, I realized that psychiatry had become wholly committed to the biological model and to drugs and electroshock. I spent two years at NIMH working on building and staffing mental health centers and then in mental health education. Then I went into private practice with no plan for becoming an active reformer as I had been in college. Then in the early 1970s, I discovered that lobotomy and newer forms of psychosurgery were being advocated and even promoted throughout the world, including the United States, Canada and Europe. I was outraged and decided to conduct what became an international campaign that stopped the worldwide resurgence of lobotomy and psychosurgery on adults and children. Eventually all but a handful of projects around the world were forced to stop and all psychosurgery came to halt in federal and state institutions in the United Sates.
The anti-psychosurgery campaign was a major project, at times all-consuming, that required many hours of volunteer work per week for several years. The successful reform effort is described in a chapter in the War Against Children of Color (1998, coauthored by Ginger Breggin), and in the Special Topics section on this website under the topic of “Psychosurgery” as well as the topic of “Racism and Social Control.”
~ Taken from http://www.breggin.org/
The Brain-Disabling Model of Psychiatry: A Conceptual Primer for Students
This information came from Dr. Breggin’s book “Brain-Disabling Treatments in Psychiatry: Drugs, Electroshock, and the Psychopharmaceutical Complex”
In the second edition of Brain-Disabling Treatments in Psychiatry, Dr. Peter R. Breggin challenges the fundamental legitimacy of modern biological psychiatry by arguing that all psychiatric interventions—including drugs, electroshock, and lobotomy—function not by curing disease, but by inducing generalized brain dysfunction. He posits that these “treatments” achieve their intended effects through deactivation, a process that suppresses higher human functions such as autonomy, self-awareness, and emotional sensitivity, effectively acting as a chemical lobotomy. Central to his critique is the concept of medication spellbinding, or intoxication anosognosia, wherein patients become unable to perceive the extent of their own drug-induced impairment, often believing they have improved while their cognitive and social health actually deteriorates. Breggin meticulously documents how the psychopharmaceutical complex promotes myths of “biochemical imbalances” to justify the use of neurotoxic substances that actually create the very imbalances they claim to treat. Ultimately, the text serves as both a scientific indictment of the industry’s deceptive marketing and a clinical guide for ethical alternatives, emphasizing a moral foundation for psychotherapy and the necessity of supervised drug withdrawal.
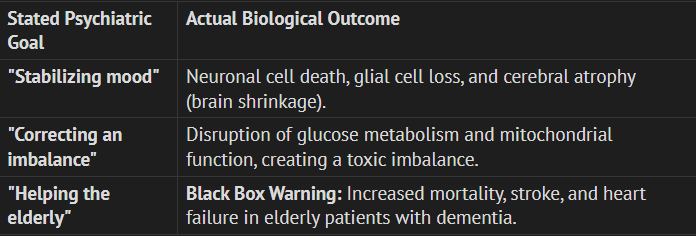
Introduction: Beyond the “Chemical Imbalance” Myth
The clinical consensus you have been taught throughout your medical education—that mental suffering is the result of a “chemical imbalance”—is an industry-sponsored fiction. In the traditional medical model, we are told psychiatric drugs act like insulin for a diabetic, correcting a pre-existing biological defect. However, Dr. Peter Breggin’s brain-disabling model reveals a far more disturbing reality: psychiatric disorders have no proven biological markers. There is no blood test, no genetic scan, and no chemical profile that can identify a patient with “schizophrenia” or “depression” before the drugs are introduced.
Key Insight:
Despite centuries of research, no commonly diagnosed psychiatric disorder has been proven to be genetic or biological in origin. The “imbalances” we see in patients are not the cause of their suffering; they are the result of the drugs. The brain is healthy until we introduce neurotoxic agents that force it to physically compensate for the resulting disability.
To grasp the mechanism of these treatments, we must abandon the myth of the “magic bullet” and examine the Basic Four Principles of how these interventions actually achieve their results through the disruption of normal function.
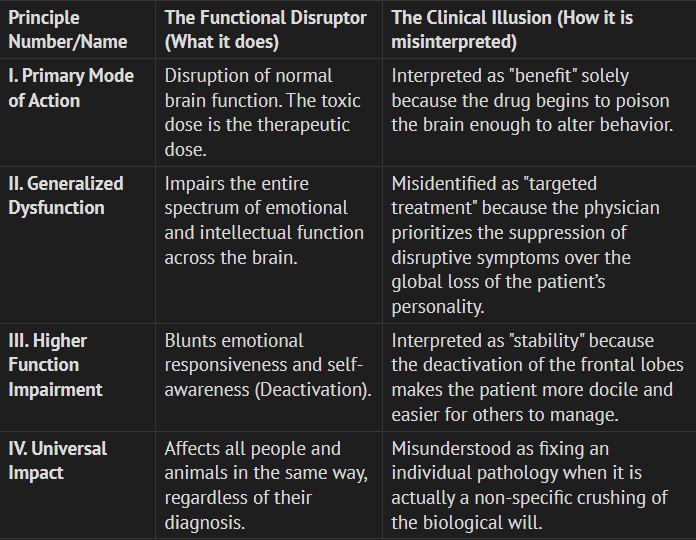
The Framework: The Basic Four Brain-Disabling Principles
All biopsychiatric treatments share a common mode of action: they achieve their “therapeutic” goals by disabling the brain. The illusion of improvement is almost always a result of the patient being rendered less capable of expressing—or caring about—their distress.
The transition from the mind of a suffering person to the mind of a “patient” is characterized by this biological response to toxicity, where the brain’s higher centers are systematically deactivated.
Disruption vs. Correction: The “TV Analogy” of the Mind
To help you understand why disabling the brain is an unethical tool for addressing human suffering, consider the analogy of a television or a computer.
The Hardware: This is the physical brain—the wiring, the circuitry, and the biological structure.
The Programming (Software): This represents our life experiences, personal biography, and our complex emotional responses to the world.
If a television program is offensive or irrational, it does not mean the “hardware” is broken. In the vast majority of psychiatric patients, neurological and neuropsychological testing indicates normal brain function until the treatments begin. This baseline of health is the absolute starting point for most sufferers. To “fix” the software (emotional pain) by smashing the hardware (disabling the brain) is a categorical error. If the hardware is disabled, the software—the thoughts, feelings, and humanity of the individual—simply cannot run.
Three reasons a person can be “disturbed” without a “broken brain:”
Natural Capacity for Stress: Human beings have a built-in capacity for extreme reactions—including losing touch with reality—when under overwhelming environmental or internal stress.
Personal Biography: Emotional distress is a reflection of an individual’s life story in all its subtle complexity, not a genetic defect.
Absence of Biological Markers: No physical illness—such as fever, lab signs, or degenerative indicators—exists in these patients until drug toxicity is introduced.
This hardware-disabling effect is not just theoretical; it is visible in every PET scan performed on medicated patients.
Scientific Grounding: Evidence of Deactivation and Suppression
Scientific evidence, particularly studies of the neuroleptic Risperdal (risperidone), provides a concrete sequence of how we deactivate a human being. The frontal lobe is the seat of “drive, motivation, and will.” By targeting this area, psychiatric drugs do not heal; they perform a functional destruction of the patient’s humanity.
The Sequence of Brain Response to Neuroleptics:
Blockade of D2 Receptors: The drug binds heavily to receptors in the emotion-regulating centers.
Metabolic Suppression: PET scans show a single dose leads to immediate metabolic suppression in the frontal lobes and limbic system.
Global Suppression of Spontaneity: Over several weeks, this produces a “Chemical Lobotomy”—a state of apathy and indifference where the patient no longer has the mental vitality to care about their symptoms.
This deactivation is why a patient may stop reporting hallucinations; they have simply been rendered too indifferent to their own existence to notice them. If the drugs are this disabling, why don’t patients protest more loudly?
The Trap of Medication Spellbinding (Intoxication Anosognosia)
Medication Spellbinding is a biological phenomenon—linked specifically to frontal lobe impairment—that renders a patient unable to recognize their own drug-induced decline.
“Why would I ever ask for forgiveness if I’ve never done anything wrong?” ~ Donald Trump
To understand this, consider the Alcohol Analogy: An intoxicated person is often the last to realize they are behaving badly or are too impaired to drive. They feel they are “doing great” even as they stumble. Psychiatric drugs work on this same principle of Intoxication Anosognosia. (I think this could be said for anybody who experiences drug / substance addiction and is arguably the reason why “The Love of Money is the Root of All Evil”)
Failure to Perceive Impairment: The individual cannot see that their emotional and mental life has been diminished.
Student Note: This biological “blindness” means the patient cannot provide true informed consent, as they are incapable of monitoring their own loss of function.
Rationalization of Distress: The individual blames negative drug effects on their “illness” rather than the medication.
Student Note: This is the “trap.” The patient may actually ask for more medication because they have been spellbound into believing their drug-induced collapse is a “relapse.”
The Illusion of Efficacy: A person may experience euphoria or a “high” that masks the fact that their social and cognitive functioning is deteriorating.
Student Note: Physicians often mistake this drug-induced mania for a “successful” lift in mood.
Medication Madness: In extreme cases, the drug drives the individual to carry out disastrous, out-of-character actions (suicide or violence) without grasping the consequences.
Student Note: The brain’s self-monitoring system is so disabled that the person acts without the “software” of conscience or judgment.
The Cost of “Improvement:” Toxicity and Cellular Death
The brain-disabling model is supported by the neurotoxic nature of these drugs. Research, including primate studies, shows that “maintenance” doses lead to significant physical brain shrinkage.
Biological Mechanism of Cell Death: Neuronal cells rely exclusively on glucose metabolism. Psychiatric drugs disrupt the mitochondria (the cell’s power plant) and glucose metabolism, leading to cellular starvation and death. In primate studies, exposure to drugs like Haldol and Zyprexa resulted in an 8% to 11% reduction in brain weight, with massive losses in both gray and white matter.
Conclusion & Summary
The choice between the “Medical Model” and the “Brain-Disabling Model” is not merely a clinical preference; it is an ethical dividing line. The Medical Model views these toxins as nutrients; the Brain-Disabling Model recognizes them as disruptors that crush the biological foundation of the soul.
As future practitioners, you must recognize that if there is no “broken brain” to fix, then disabling a healthy brain is a violation of the Hippocratic Oath. Shifting toward drug-free therapy and empathy is not just an alternative—it is a moral requirement for any practitioner who accepts the evidence of metabolic suppression and brain shrinkage.
Key Points to Remember
Function through Disability: Psychiatric drugs do not fix imbalances; they work by impairing normal brain function to produce a more manageable patient.
The “Deactivation” Goal: The “therapeutic effect” is the production of apathy and the suppression of the will (chemical lobotomy).
Compensatory Mechanisms (Principle VIII): The brain reacts to these toxins by creating new, often permanent abnormalities as it attempts to fight the drug’s disabling effects.
The Spellbinding Trap: Because the frontal lobes are impaired, the patient is biologically unable to perceive the harm, often blaming themselves for the drug’s toxic effects.

